
Why Wait to Evaluate?
03/07/2020 | Ann Marie Hofbauer, DMD
Scaling and Root Planing: A Refresher of Evidence
We complete scaling and root planing nearly on a daily basis and constantly remind our patients to return in 4-8 weeks for a periodontal re-evaluation, but why? Have you ever wondered about the origins of this recommended timeline?
If yes, this is the post for you.
Morrison, Proye, Magnusson, Lowenguth and Greenstein are to thank for
elucidating the ideal timeframe for healing after scaling and root planing (S/RP).
In 1980 Morrison et al1 observed pocket reduction and improvement in attachment levels 4 weeks after completing the “hygienic phase” of therapy which included S/RP, oral hygiene instructions, and occlusal adjustments. Morrison’s group noted that the need for periodontal pocket reduction surgery cannot be appropriately assessed until after completing the “hygienic phase of therapy”.
Then in 1982 Proye, Caton, and Polson2 showed an improvement in clinical attachment at 3 weeks, but observed no additional clinical attachment gain in the following 12 weeks. This trio noted significant initial pocket depth reduction 1 week after S/RP, but further reduction was noted when re-evaluation was delayed until 3 weeks. The initial reduction at 1 week was associated with gingival recession, while the secondary reduction at 3 weeks was associated with gain of attachment.
In 1984 Magnusson et al3 observed the bacterial composition of subgingival plaque pre- and post-S/RP. This group noted that in the presence of supra-gingival plaque the composition of subgingival bacteria will return to baseline levels 4-8 weeks after S/RP. Magnusson explained that at 8 weeks post-S/RR bacterial recolonization will plateau in the absence of adequate oral hygiene, meaning 8 weeks after S/RP our periodontitis patients will become susceptible to further disease progression. This is why we plan to re-evaluate prior to the 8-week time point — to prevent further attachment loss.
Lowenguth and Greenstein4 reviewed the clinical and microbiologic response to S/RP in 1995 and found that re-evaluation should occur at a minimum of 3-4 weeks after therapy to allow for soft tissue healing and maturation. Furthermore, the authors note that optimal soft tissue healing and maturation around teeth occurs between 4 and 8 weeks.
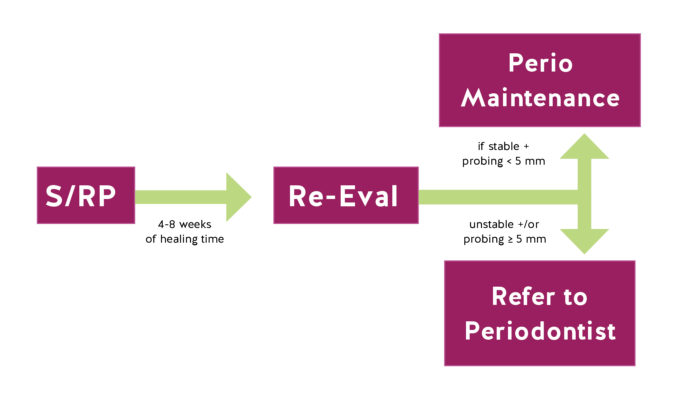
Combining the work of these authors we can reasonably proceed with planning periodontal re-evaluations 4-8 weeks after S/RP. If we re-evaluate too soon we risk evaluating a patient who has not completely healed, which may promote over-treatment. Conversely, if we re-evaluate too late further disease progression may occur and our therapy will not be optimized. Additionally, this time allows patients the opportunity to improve their home care and develop new oral hygiene habits.
A re-evaluation 4-8 weeks after S/RP will provide an accurate assessment of the patient’s periodontal status and their potential need to see a periodontist. Carranza’s Clinical Periodontology5 reviews the decision of when to refer to a specialist at a periodontal re-evaluation and notes that this decision can be guided by the 5-mm standard. According the Carranza,
“The rationale behind the 5-mm standard is that the typical root length is about 13 mm and the crest of the alveolar bone is at a level approximately 2 mm apical to the bottom of the pocket. When there is 5 mm of clinical attachment loss the crest of bone is about 7 mm apical to the cementoenamel junction, therefore only about half the bony support for the
tooth remains. Specialist care can help preserve teeth in these cases by eliminating deep pockets and regenerating support for the tooth.”
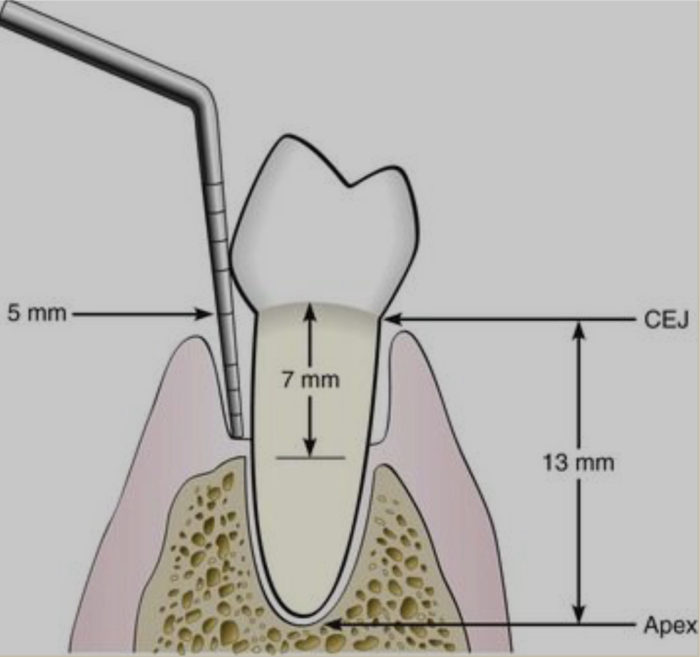
Figure 43-4 From Carranza’s Clinical Periodontology depicts the relationship of 5 mm of clinical attachment loss to tooth support.
Treating periodontitis is generally successful in patients with probing depths less than 7 mm but success rates decrease when probing depths exceed 9 mm, therefore early referral of patients prior to disease advancement is pivotal for maintaining the dentition in periodontitis patients.
References:
- Morrison EC, Ramfjord SP, Hill RW. Short-term effects of initial, nonsurgical periodontal treatment (hygienic phase). J Clin Periodontal 1980; 8: 199-211.
- Proye M, Caton J, Polson A. Initial healing of periodontal pockets after a single episode of root planing monitored by controlled probing forces. J Periodontal 1982; 53: 296-301.
- Magnusson J, Lindhe T, Yoneyama, Liljenberg B. Recolonization of a subgingival microbiota following scaling in deep pockets. J Clin Periodontal 1984; 11: 193-207.
- Lowenguth RA, Greenstein G. Clinical and microbiological response to nonsurgical mechanical periodontal therapy. Periodontol 2000 1995; 9: 14-22.
- Newman, Michael G.; Takei, Henry; Klokkevold, Perry R.; Carranza, Fermin A.. Carranza’s Clinical Periodontology (Newman, Carranza’s Clinical Periodonyology) (Kindle Locations 42471-42479). Elsevier Health Sciences. Kindle Edition.






